tree in bud opacities treatment
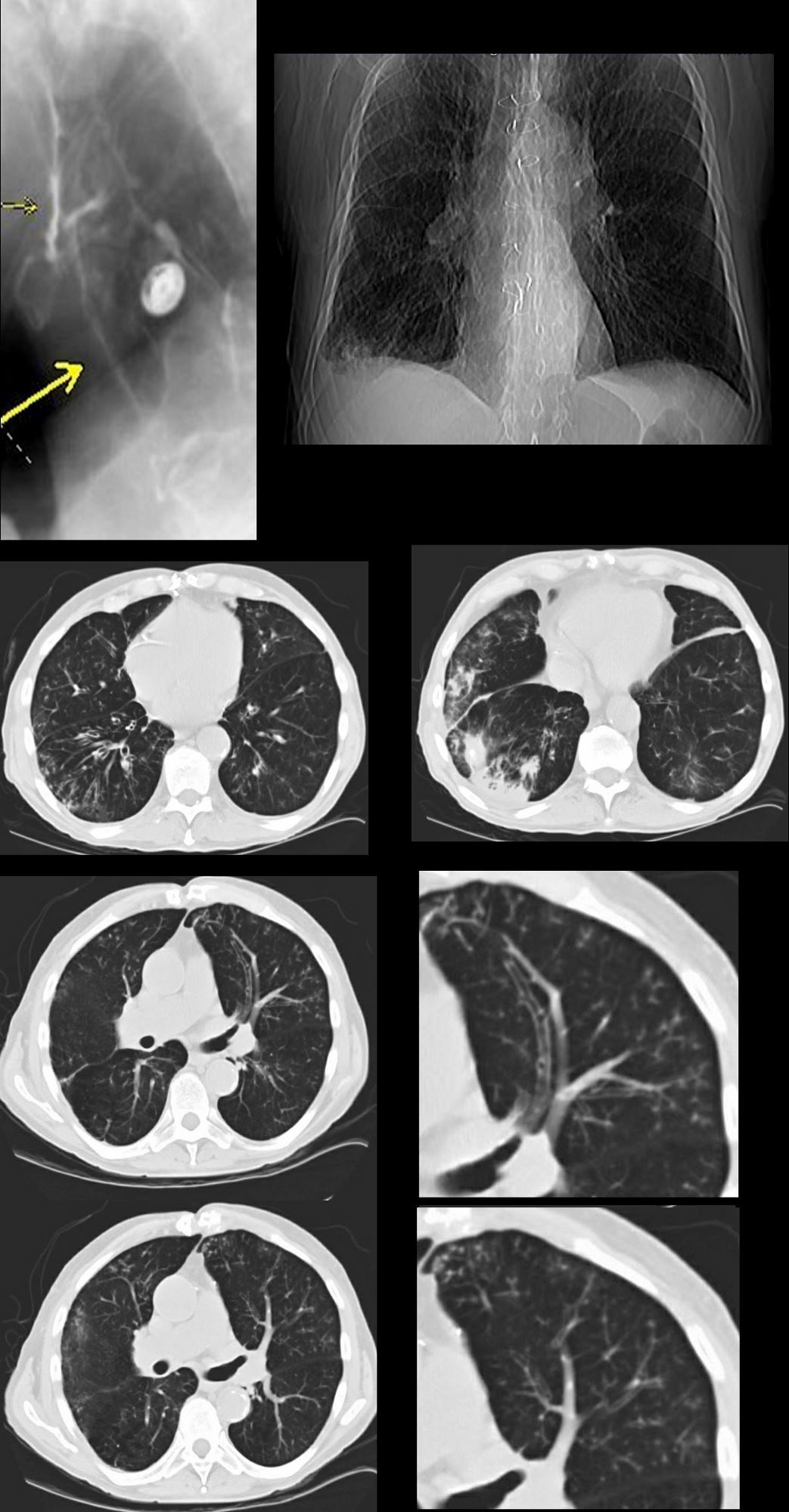
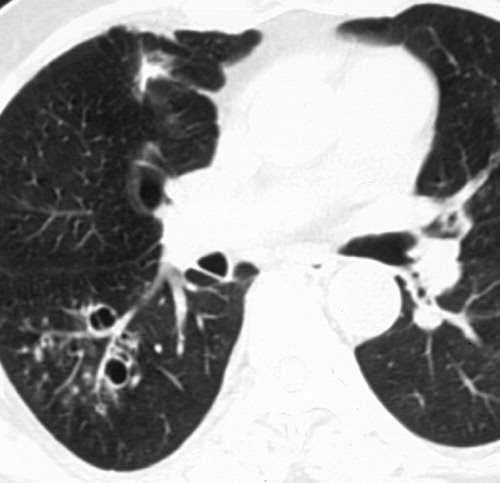
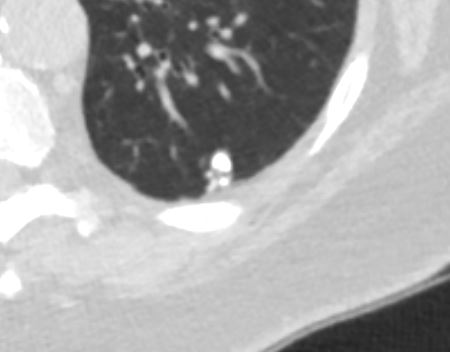
High-resolution CT scan of the thorax demonstrates central bronchiectasis a hallmark of allergic bronchopulmonary aspergillosis right arrow and the peripheral tree-in-bud appearance of centrilobular opacities left arrow which represent mucoid impaction of the small bronchioles. The lesion was so named because of its bulbous appearance and characteristic focal areas of reddish-blue discolouration from venous channels that resemble an eye at arthroscopy.

Tree In Bud Pattern At Thin Section Ct Of The Lungs Radiologic Pathologic Overview Radiographics
Cryptogenic organizing pneumonia 119.

. Treatment and prognosis. Adjacent bronchial wall thickening is also frequently depicted. Classically bronchiolitis appears as a region of centrilobular nodularity often in a tree-in-bud pattern.
Either centrilobular nodules or opacities well defined lesions 2 to 4 mm separated by 2 mm from the pleural surface or interlobular septa with or without tree-in-bud. A recent small study of nine patients with M. A high-resolution CT HRCT is more sensitive to changes such as bronchiectasis small nodules tree-in-bud appearance ground-glass opacities and pleural thickening.
With centrilobular nodules and tree-in-bud pattern in relation to the bronchiectasis. Treatment and prevention of nontuberculous mycobacterial diseases. A significant radiologic finding in chest CT is the tree-in-bud pattern consisting of multiple branching linear structures that represent bronchogenic dissemination of disease.
They refer to struvite calculi involving the renal pelvis and extending into at least two calyces 7. The nodules develop rapidly into cavities within days. Kansasii described primarily nodules bronchiectasis and tree-in-bud opacities detected by computed tomography with cavitation in only four 44 cases.
Allergic bronchopulmonary aspergillosis ABPA is a fungal infection of the lung due to a hypersensitivity reaction to antigens of Aspergillus fumigatus after colonization into the airways. Endobronchial spread along nearby airways is a relatively common finding resulting in relatively well-defined 2-4 mm nodules or branching lesions tree-in-bud sign on CT 13. An unusual pattern similar to the nodules seen in subacute.
Mild focal or unilateral abnormality is also regarded as equivocal for ILA. When compared to pulmonary tuberculosis upper lobe cavitation is less common and middle lobe bronchiectasis more frequent in Mycobacterium avium complex pulmonary infections. For prominent cysts consider.
It represents dilated and impacted mucus or pus-filled centrilobular bronchioles. Tiddens HAWM Meerburg JJ van der Eerden MM Ciet P. Other non-ILA findings include focal paraspinal fibrosis in close contact with spine osteophytes interstitial edema eg as in heart failure and findings of aspiration such as patchy ground-glass and tree-in-bud opacities Table 3 and Fig 5.
Branching opacities cavitation or consolidation are clear signs of active TB but active disease must be confirmed by analyzing sputum for the presence of bacilli. This involves the creation of an interatrial baffle to redirect the pulmonary venous return into the left atrium. The clinical and CT findings of numerous respiratory viral pathogens such as influenza human parainfluenza virus HPIV respiratory syncytial virus RSV rhinovirus and adenovirus have been described 12RSV shows an airway-centric pattern of disease with tree-in-bud opacity and bronchial wall thickening.
It characteristically presents with bronchospasm pulmonary infiltrates eosinophilia and. Findings consistent with other infections like typical bronchiolitis with tree-in-bud and thickened bronchus walls tbc. Tree in bud opacity.
Treatment and prognosis. Kansasii is a significant cause of pulmonary disease among persons with advanced human immunodeficiency virus infection. No typical signs of COVID-19.
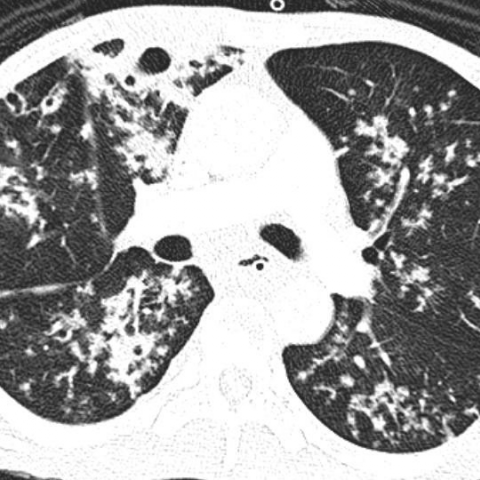
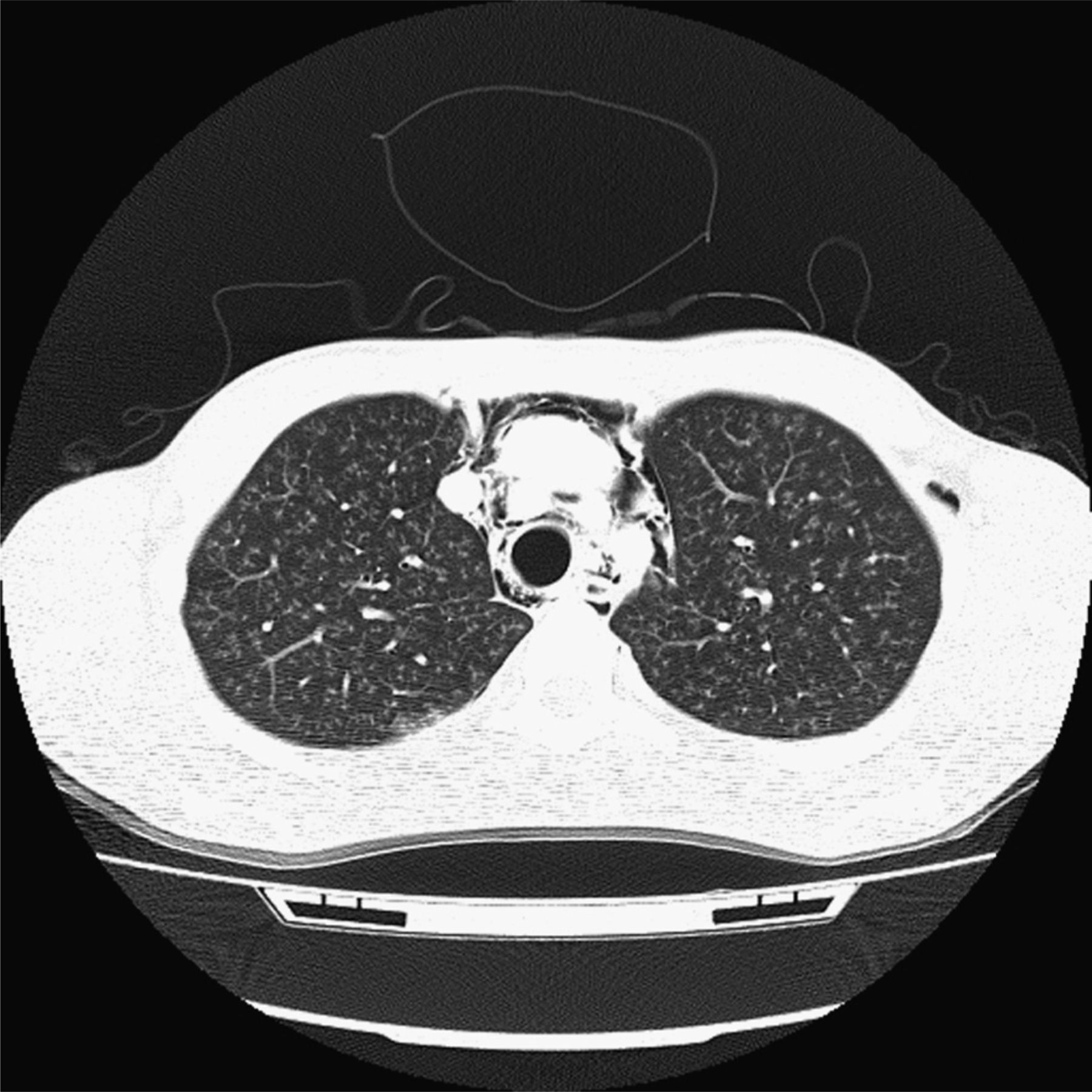
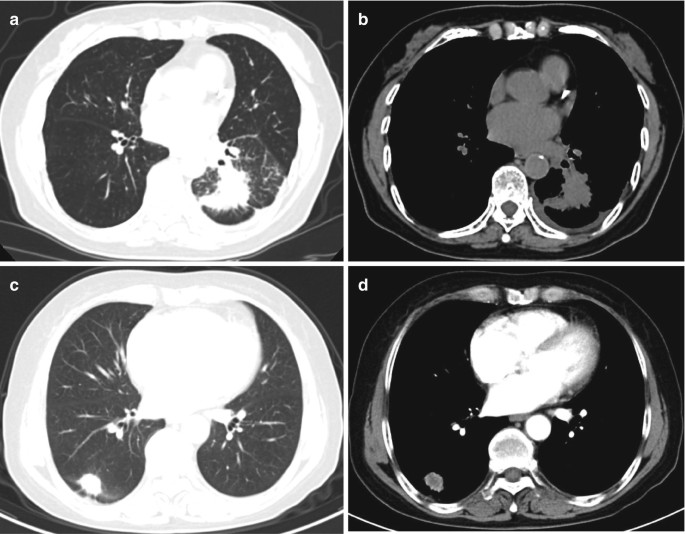
In the right mid-lung nodular opacities are in a tree-in-bud distribution suggestive of endobronchial spread. The development of an air-fluid level implies communication with the airway and thus the possibility of contagion. For a general discussion of renal calculi please refer to nephrolithiasis.
The CT presentation consists of multiple peripheral nodular or wedge-shaped opacities with a broad base against the pleura. Surgical correction should be considered in the presence of significant left to right shunting and pulmonary hypertension. Immune reconstitution inflammatory syndrome IRIS.
Alternatively the anomalous vein can be re-implanted directly into the left atrium. Predominantly it affects patients with bronchial asthma and those having cystic fibrosis. Right Coronal NECT MIP image of the same patient shows bronchiectasis mucoid impactions st and tree-in-bud opacities from bronchiolar mucoid impactions.
Those larger than 25 mm in the maximal dimension are called giant cerebral aneurysms. Treatment with tumor necrosis factoralpha TNF-α antagonists which is used for rheumatoid arthritis psoriasis. Visible thickened visceral and parietal pleura with fluid collection in between Suggests the presence of empyema.
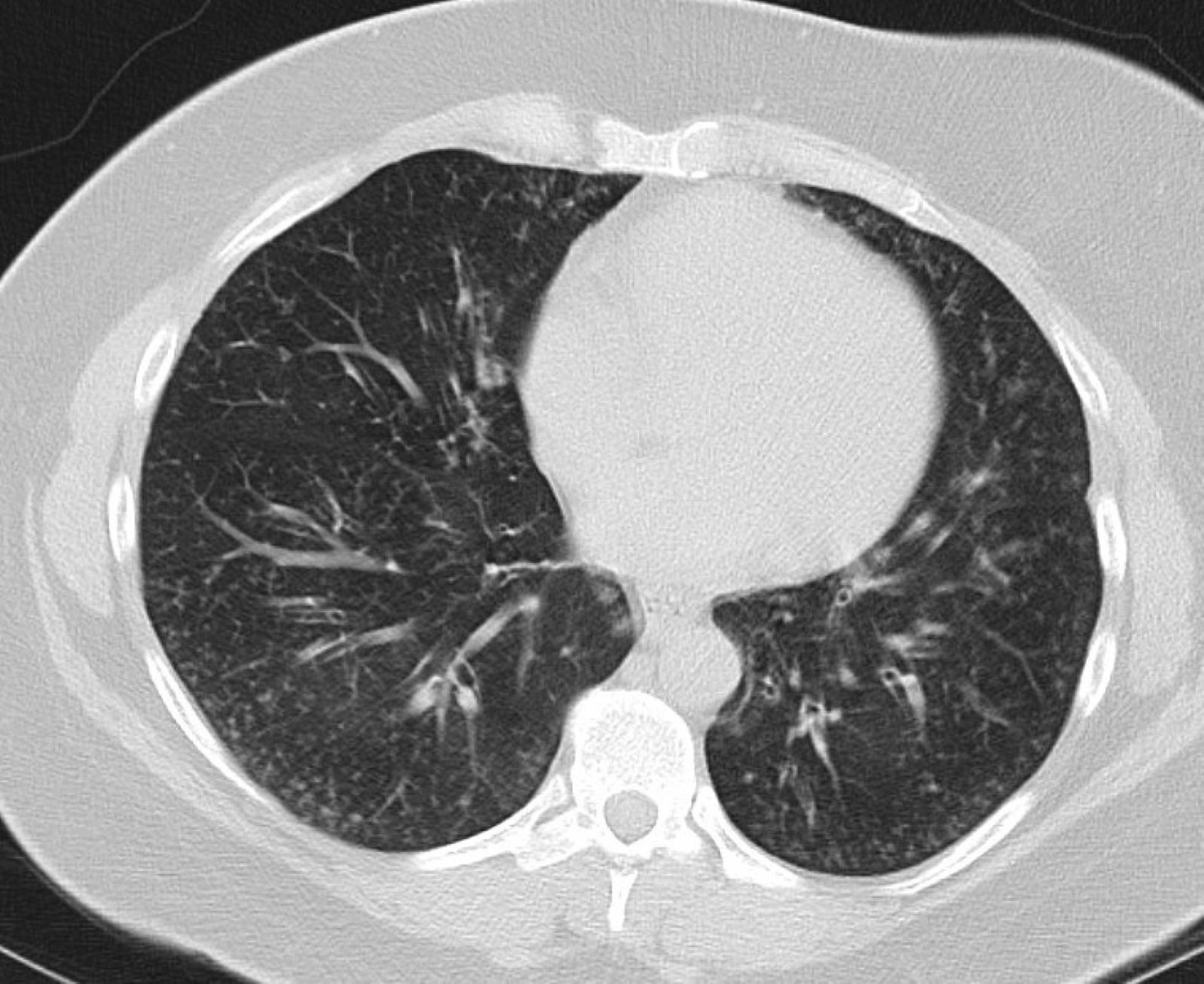
Charcot-Bouchard aneurysms are minute aneurysms which develop as a result of chronic hypertension and appear most commonly in the basal ganglia and other areas such as the thalamus pons and cerebellum where there are small penetrating vessels. There are no ground glass opacities. Poorly defined centrilobular nodules and tree-in-bud pattern.
Associated focal ground-glass and consolidative opacities may be visualized although this should not the predominant feature. Visible small airways or terminal bronchioles filled with mucus pus fluid or cells forming impactions that resemble a budding tree with branching nodular V and Y shaped opacities Split pleura sign. Causes and imaging patterns of tree-in-bud opacities.
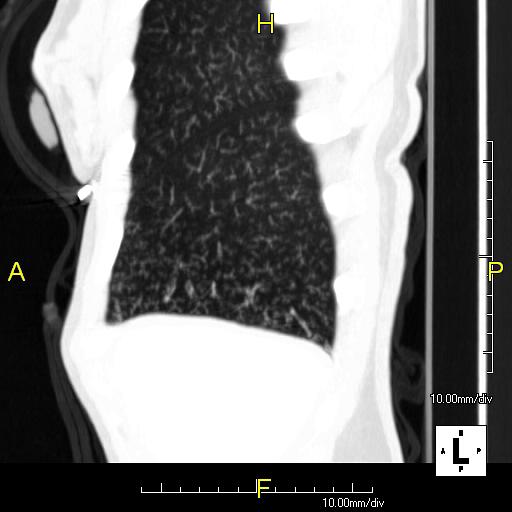
Various viral pneumonias 232 especially postbone marrow transplant 173. Tree-in-bud describes the appearance of an irregular and often nodular branching structure most easily identified in the lung periphery. In centrilobular nodules the recognition of tree-in-bud is of value for narrowing the differential diagnosis.
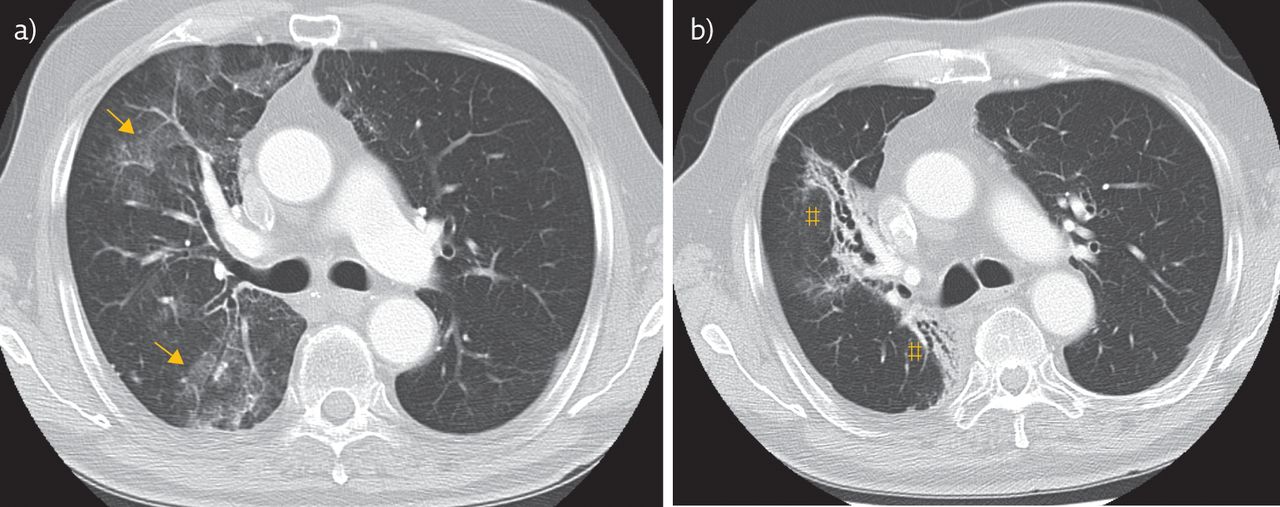
Patients receiving antiretroviral therapy ART Other conditions to be considered which also occur in non-AIDS patients include. A 57-year-old man with polyarteritis nodosa was evaluated for cough and pulmonary opacities. Cylindrical bronchiectasis is more common in asthma and cystic or varicoid bronchiectasis is more common in allergic bronchopulmonary.
The CT-image shows bronchiectasis bronchial wall thickening and tree-in-bud arrows. Indirect signs of small airways disease include a mosaic pattern of attenuation on inspiratory CT scan and air trapping on expiratory CT scan. Centrilobular nodules tree-in-bud pattern ground-glass opacities and consolidation.
Chest CT revealed multifocal clustered centrilobular nodules and opacities in a tree-in-bud pattern. Treatment is arthroscopic excision. When upper zone cysts are prominent and if tree-in-bud opacities are present.
Opacities that represent mucoid impactions st. Small patchy peripheral opacities are also present in the left lower lobe. Direct signs of small airways disease include ill-defined centrilobular nodules and well-defined centrilobular branching nodules also called tree-in-bud opacities which may be best seen using MIP.
Staghorn calculi also sometimes called coral calculi are renal calculi that obtain their characteristic shape by forming a cast of the renal pelvis and calyces thus resembling the horns of a stag.

Causes And Imaging Patterns Of Tree In Bud Opacities Sciencedirect
Tree In Bud Sign Wikipedia

Tree In Bud Sign Lung Radiology Reference Article Radiopaedia Org

Tree In Bud Sign An Overview Sciencedirect Topics
Tree In Bud Pattern Pulmonary Tb Eurorad
Cureus Follicular Bronchiolitis Associated With Primary Igg2 Igg4 Deficiency In A Previously Healthy 40 Year Old Woman

Tree In Bud Pattern At Thin Section Ct Of The Lungs Radiologic Pathologic Overview Radiographics
Tree In Bud Sign Lungs
Tree In Bud Sign Lungs

Causes And Imaging Patterns Of Tree In Bud Opacities Sciencedirect
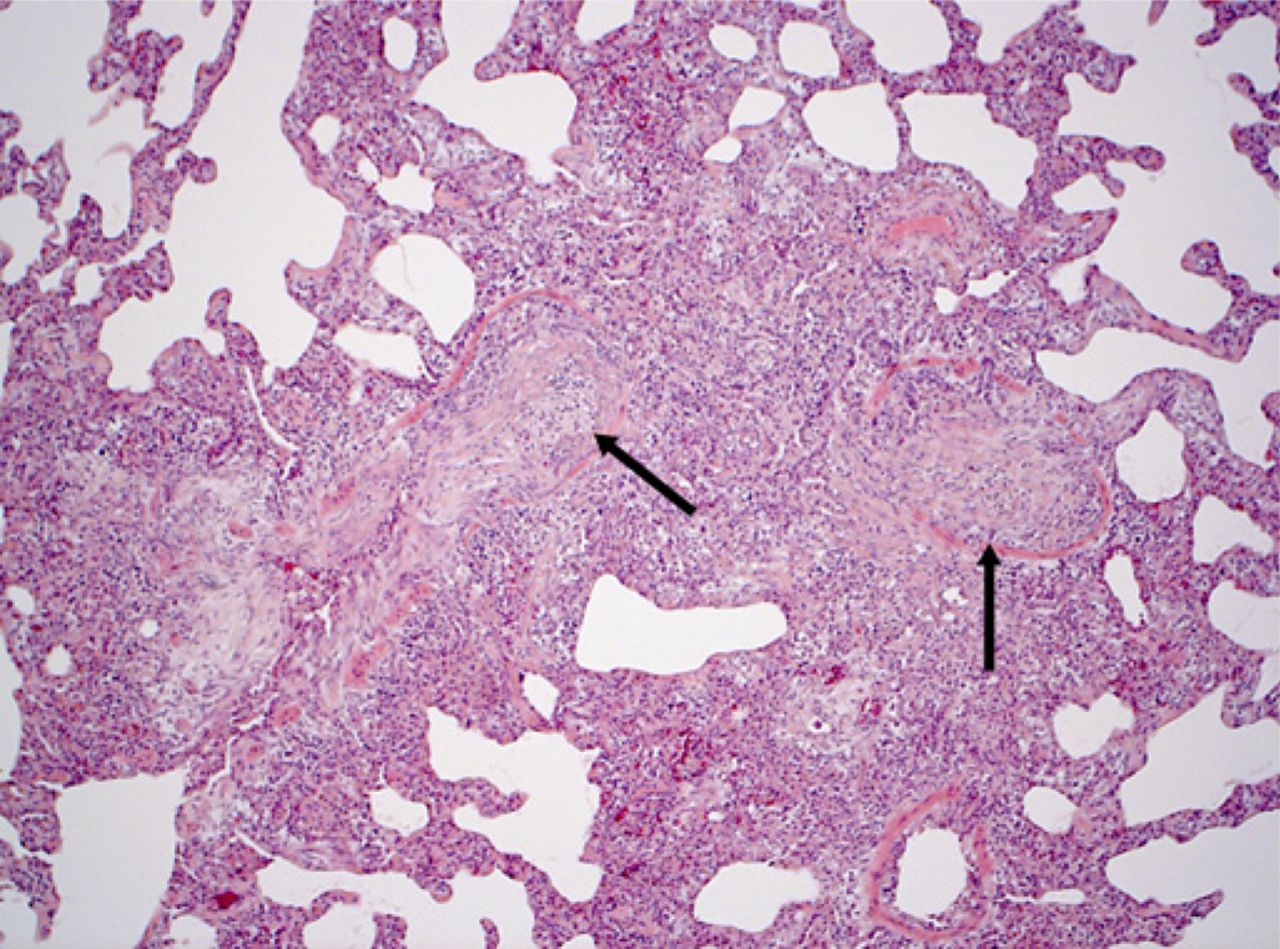
Tree In Bud Attributable To Organising Pneumonia Thorax
Diagnostic Imaging In Adult Non Cystic Fibrosis Bronchiectasis European Respiratory Society
Tree In Bud Attributable To Organising Pneumonia Thorax
Tree In Bud Sign Lungs

Tree In Bud Opacities Most Prominent In The Right Middle Lobe Due To Download Scientific Diagram

Tree In Bud Pattern In Central Lung Cancer Ct Findings And Pathologic Correlation Sciencedirect

Tree In Bud Pattern At Thin Section Ct Of The Lungs Radiologic Pathologic Overview Radiographics
Chest Springerlink

Scielo Brasil Tree In Bud Pattern Tree In Bud Pattern